""""""""""""""""""""""""""""""""""""""""""""""" the Ottawa Ankle Rule
Stiell and colleagues developed the concept of a clinical decision rule to guide the assessment of ankle injuries—in particular, to determine the indications for radiography.This became known as the Ottawa ankle rules, using bony tenderness and inability to bear weight as positive indicators for radiography.
Sensitivities for the Ottawa Ankle Rule range from the high 90% to 100% range for “clinically significant” ankle and midfoot fractures. This isdefined as a fracture or an avulsion > 3 mm.
Specificities for the Ottawa Ankle Rule are approximately 41% for the ankle and 79% for the foot, although the rule is not designed or intended to make a specific diagnosis.
The Ottawa Ankle Rule is useful in ruling out fracture (high sensitivity), but does poorly at ruling in fractures (many false positives) and its use should reduce the number of unnecessary radiographs by 30-40%
ankle sprain Updated: Jan 14, 2019 https://emedicine.medscape.com/article/1907229
Provide patients with information on when to call for advice if one of the following conditions is observed: - The joint is wobbly or moves past its normal ROM - The bone is deformed or bends abnormally - Pain prevents putting weight on the injured area after 24 hours - Weight-bearing still is difficult after 4 days - Extreme pain, bruising, or severe swelling is present - The toes below the injury feel cold to the touch or become numb or blue
In a systematic literature review, 36-85% of patients with acute ankle sprains reported full recovery at 2 weeks to 36 months,independent of the initial grade of sprain,with most recovery occurring within the first 6 months. After 12 months, the risk of recurrent ankle sprain returns to preinjury levels.However, 3-34% of patients reported re-sprains at 2 weeks to 96 months after the initial injury. Furthermore, after 3 years, some patients still had residual pain and instability. One risk factor for residual symptoms seems to be participation in competitive sports.
Functional instability of the ankle has been defined variously as the occurrence of frequent sprains, difficulty running on uneven surfaces, difficulty cutting or jumping, and recurrent giving-way for at least 6 months despite adequate nonsurgical therapy. Instability may result from tibiotalar laxity or subtalar instability.
For recurrent lateral ankle sprains, treatment should begin with a trial of conservative therapy for approximately 2-3 months.The recurrence rate for lateral ankle sprains has been reported to be as high as 80%.
**********************************
It is generally accepted that for most patients, operative repair of third-degree anterior talofibular ligament (ATFL) tears and medial ankle ligament tears does not contribute to an improved outcome. One of the few absolute indications for surgery in patients with a sprained ankle is a distal talofibular ligament third-degree sprain that causes widening of the ankle mortise. A second indication is a deltoid sprain with the deltoid ligament caught intra-articularly and with widening of the medial ankle mortise.
In selected young patients with high athletic demands who have both anterior talofibular and calcaneofibular complete ruptures, surgical repair may be the treatment of choice.
For recurrent lateral ankle sprains, treatment should begin with a trial of conservative therapy for approximately 2-3 months , if these measures are unsuccessful, surgical intervention is necessary. In syndesmotic injuries, when a diastasis has been present for longer than 3 months .
Chronic instability of the subtalar joint frequently requires surgical intervention
********************************** Return-to-play criteria during the recovery phase (3 d to 2 wk post injury) include the following: - Full, pain-free active and passive ROM - No pain or tenderness - Strength of ankle muscles 70-80% of that on the uninvolved side - Ability to balance on 1 leg for 30 seconds with eyes closed
Return-to-play criteria during the functional phase (2-6 weeks postinjury) include the following: - Normal ROM of the ankle joint - No pain or tenderness - Satisfactory clinical examination - Strength of ankle muscles 90% of the uninvolved side - Ability to complete functional examination
Stiell and colleagues developed the concept of a clinical decision rule to guide the assessment of ankle injuriesin particular, to determine the indications for radiography.This became known as the Ottawa ankle rules, using bony tenderness and inability to bear weight as positive indicators for radiography.
Sensitivities for the Ottawa Ankle Rule range from the high 90% to 100% range for clinically significant ankle and midfoot fractures. This isdefined as a fracture or an avulsion > 3 mm.
Specificities for the Ottawa Ankle Rule are approximately 41% for the ankle and 79% for the foot, although the rule is not designed or intended to make a specific diagnosis.
The Ottawa Ankle Rule is useful in ruling out fracture (high sensitivity), but does poorly at ruling in fractures (many false positives) and its use should reduce the number of unnecessary radiographs by 30-40%
ankle sprain Updated: Jan 14, 2019 https://emedicine.medscape.com/article/1907229
Provide patients with information on when to call for advice if one of the following conditions is observed: - The joint is wobbly or moves past its normal ROM - The bone is deformed or bends abnormally - Pain prevents putting weight on the injured area after 24 hours - Weight-bearing still is difficult after 4 days - Extreme pain, bruising, or severe swelling is present - The toes below the injury feel cold to the touch or become numb or blue
In a systematic literature review, 36-85% of patients with acute ankle sprains reported full recovery at 2 weeks to 36 months,independent of the initial grade of sprain,with most recovery occurring within the first 6 months. After 12 months, the risk of recurrent ankle sprain returns to preinjury levels.However, 3-34% of patients reported re-sprains at 2 weeks to 96 months after the initial injury. Furthermore, after 3 years, some patients still had residual pain and instability. One risk factor for residual symptoms seems to be participation in competitive sports.
Functional instability of the ankle has been defined variously as the occurrence of frequent sprains, difficulty running on uneven surfaces, difficulty cutting or jumping, and recurrent giving-way for at least 6 months despite adequate nonsurgical therapy. Instability may result from tibiotalar laxity or subtalar instability.
For recurrent lateral ankle sprains, treatment should begin with a trial of conservative therapy for approximately 2-3 months.The recurrence rate for lateral ankle sprains has been reported to be as high as 80%.
**********************************
It is generally accepted that for most patients, operative repair of third-degree anterior talofibular ligament (ATFL) tears and medial ankle ligament tears does not contribute to an improved outcome. One of the few absolute indications for surgery in patients with a sprained ankle is a distal talofibular ligament third-degree sprain that causes widening of the ankle mortise. A second indication is a deltoid sprain with the deltoid ligament caught intra-articularly and with widening of the medial ankle mortise.
In selected young patients with high athletic demands who have both anterior talofibular and calcaneofibular complete ruptures, surgical repair may be the treatment of choice.
For recurrent lateral ankle sprains, treatment should begin with a trial of conservative therapy for approximately 2-3 months , if these measures are unsuccessful, surgical intervention is necessary. In syndesmotic injuries, when a diastasis has been present for longer than 3 months .
Chronic instability of the subtalar joint frequently requires surgical intervention
********************************** Return-to-play criteria during the recovery phase (3 d to 2 wk post injury) include the following: - Full, pain-free active and passive ROM - No pain or tenderness - Strength of ankle muscles 70-80% of that on the uninvolved side - Ability to balance on 1 leg for 30 seconds with eyes closed
Return-to-play criteria during the functional phase (2-6 weeks postinjury) include the following: - Normal ROM of the ankle joint - No pain or tenderness - Satisfactory clinical examination - Strength of ankle muscles 90% of the uninvolved side - Ability to complete functional examination










 ฝากข้อความหลังไมค์
ฝากข้อความหลังไมค์ ผู้ติดตามบล็อก : 762 คน [
ผู้ติดตามบล็อก : 762 คน [
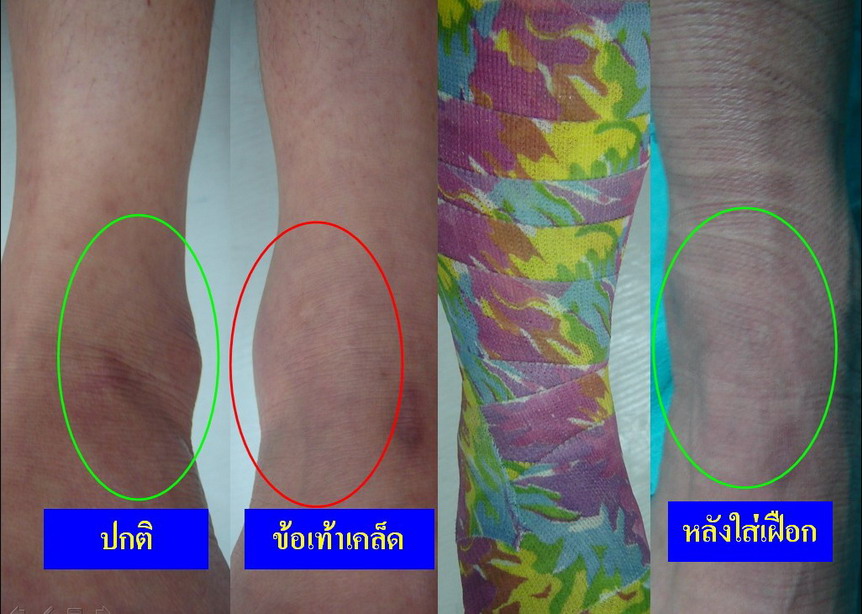
กว่าจะหาย4-6อาทิตย์เลยเหรอค่ะ นานจัง
แต่เดี๋ยวถ้ารู้สึกว่าดีขึ้นแล้วจะลองทดสอบแบบที่คุณหมอแนะนำ
ขอบคุณความรู้ดีๆที่เอามาฝากนะค่ะ