- JyHorseman Digital Sweet
- 2011m07d27: My Favourite Link
- Cyber ; Try to be there.
- Boy Double Bass, Hua-Hin
- Sivalee, Pinklao-Sathorn
- Sivalee, Turf Grasses [�Ѻ��û�١˭���ʹ�� ... �ա����]
- 2010m09d25: ��ͻ�Һ�������� (TPBS Channel)
- 2008m06d01: ��١�鹾ԡ�ŷ�᷹���Ӵ��
- 2009m11d26-28: ��١������� (���Ǻ�ҫ��)
- 2010m01d09 : �����͢�������ᡧ�ԧ (Carnivorous Plants)
- 2010m08d01: My Roses (��١����Һ)
- 2010m01d19: Ford Telstar TX4
- 2010m05d05; Nissan Teana 250XV
- 2011m11d11: The Car New Ones [����ö�����ա�ѡ�ѹ]
- 2010m06d25: My First Ones, Nikon D90
- 2010m07d23: Get Nikon D5000, 2 Lens
- 2011m01d26: Nikon Coolpix S3000, 3rd
- 2011m09d01: Tripod for DSLR [����ǡѺ�ҵ�駡��ͧ DSLR]
- 2011m12d08: Nikon Speedlight, It's the next.
- 2013m02d20: Get the New Pixel TC-252 Cable Timer Remote Control
- 2010m09d12: Training with World Camera-Ladpraw
- 2011m02d26: D2H Basic Camera Usage
- 2010m02d14: My Denali, Sundance Hot Tub Spa
- 2010m07d14: Electrical Rotary Drill BOSCH; GBH 2-26 DFR
- 2010m10d13: Electrical Drill BOSCH; GSB 10 RE
- 2010m10d11: Digital Multimeters UT33 Series
- 2011m04d28: Hidef Player [����ͧ�����ി]
- 2011m05d19: Blood Pressure Monitoring [��ͧ���ѧ����ͧ�����ѹ���Ե�٧����]
- 2012m07d23: Eggs for Blood Pressure [����ͧ��������ª���ѡ]
- 2012m01d09: My GPS Garmin nuvi 1250
- 2009m12d29-m01d03: Trip, Kunming - Jade Dragon Snow Mountain
- 2010m06d05-07: Trip, WangNamKhaew
- 2010m07d24-27: Yon-Roi iSan, OSorTho
- 2010m10d01-03: Trip Island, Thong-Pha-Phum
- 2011m02d03-07 : Trip, Angkhang - Pai
- 2011m05d04-05: Trip, Kanchanaburi-Naraesuan (�ç���¹�����)
- 2011m05d21,28 & m06d04_Trip, MuseumSiam, Yutha-Sarth
- 2011m08d18, m09d02-04&18: OSoTho, Writer & Photographer Project
- 2011m10d15-16: Trip, Nissan Teana Family Caravan [�����ҹ ����� ����� �����ѹ]
- 2012m02d99: Let's Trip at Kangkrajan [��Ի, �觡�Шҹ]
- 2012m07d13-15: Foto Trip, ��-���-�� ���ͧ�Ѻ�� ���Ȩ���������ҹ��ѧ��
- 2010m11d30: Nurse
- 2010m12d13: Ancientism Collection
- Water Sport, JetSki & JetBoat
- JyHorseman Sweet Trip
- 2011m02d22: Archery Horseman
- 2011m05d25: Golf Training
- 2011m06d13: Ukulele Guitar, The New Ones
- 2012m02d25-m04d08: ������¹�����Ҿ�����Ҫվ ��� 50
- 2012m11d24: SEAL @Thonburi [���, ��ӽ�觸����Ѵ������� ...]
- 2012m12d07-10: Trip Nan [������ҹ, �Ե������ ������ʹ�� �Ҫ�� ����٤� �������]
- 2012m12d21-25: Trip ZhangJiaJie [�������ǵ�� �ҧ�� �ҧ��������]
- 2012m12d28-2013m01d02: Trip Lao [����˹��, ���§�ѹ���, �ѧ���§, ��ǧ��кҧ]
- 2013m01d10: Photographer Favorite Tips & Technics
- 2013m01d26-27: Relaxation Time at Rayong
- 2013m03d02: D2H Training, Concert Activity Take Shot [ͺ����ö����Ҿ�ҹ������]
- 2013m03d09: Trip Klong Bang Luang [��ͧ��ͧ�ҧ��ǧ ������������]
- 2013m03d30-31: EyeContact 02-Workshop "Star Trail" with DSLR at Pangsida
- 2013m02d22: Time Lapse with Nikon DSLR
- 2013m02d23: ��ö����Ҿ��ͧ��������Ӥ
- 2013m03d18: DengoTech Tablet PC A79, The New Ones
- 2013m05d17: Got 2 Nikon Lens, 50 mm. F1.8G & 18-200 mm.
- 2013m06d14: LG LM6200 3D TV - Lighting on Screen [�ʧ����˹�Ҩ��Ҿ]
- 2013m06d15: �������ʶҹ�ѧ��� "�ѧ����ʡ�ѹ - �Ѵອ����Եô��Եǹ����"
- 2013m08d31: Picture for Products by Digital2Home [��ö����Ҿ�Թ��� �� D2H]
- 2013m11d02: Travel and Documentary Photography - 2nd Group [��ö����Ҿ������ä�շ�ͧ����� �������� 2]
- 2013m11d03: Basic Photographic Techniques by EyeContact [ͺ����鹰ҹ��ö����Ҿ���ͧ��]
- 2013m11d19-23: Korea Trip - Rapid Tour [���������� - �������,����觴�ǹ]
- 2013m12d24: Wire for RJ Lan Plug [������§�ӴѺ���俢ͧ�����Ź��]
- 2013m12d27: New Luggage, How to ? [���͡������Թ�ҧ�����, ���ҧ�ô�]
- 2014m02d05: Get Katana Sword - Snipe Wood SF-1
- 2014m02d22: Koh-Kred Trip with Variety Siam [��Ի������ �Ѻ�����ԾԸ����]
- 2014m03d13-15: Myanmar Trip [Yangon-Sirieam-Hongsawadee]
- 2014m11d13-16: Myanmar Trip [Phukam-Mandalay]
- 2014m03d28-30: Uthathani Trip with Variety Siam [�����ѡ�ط�¸ҹ�]
- 2014m04d12-15: Jeju Island, South Korea with TourTook
- 2014m04d24: Nikon School - Flash Workshop
- 2014m04d26-27: Sri-Chang Island with Variety Siam ["�ժѧ" ����Ҫ�ҹ��觤����ç��㹾�оط������ǧ]
- 2014m05d28: Playing Golf with JyHorseman
 - 2014m06d15: Maria Na KraiBaan [Nikon Workshop - I am Happy Living]
- 2014m07d17: Let's JyHorseman Trips
- 2014m12d09: Learning Golf by Yourself with Pro Chaowarat [�֡�������쿴��µ��ͧ�Ѻ������ѵ��]
- 2015m01d11: Get in the Turntable & Gramophone Record [����ͧ��������§]
- 2015m01d11: Jyhorseman Turntable Shelf
- 2014m12d30-2015m01d03: Trip South of Lao [����ѹ⺡-�����-⢧����-�����]
- 2015m06d13-15: Chanthaburi Trip with Father
- 2015m10d14-15: Adobe Photoshop CS6 Class Training
- 2015m11d28-m12d02: Trip Japan [Tokyo, Fuji] with Chill Square Travel
- 2016m02d25-26: SketchUp 2014 and Basic V-Ray Training
- 2016m03d11: Callaway Golf in My Games
- 2016m12d29-2017m01d01: Vietnam Trip
- 2017m01d01: My Golf Bags
- 2017m04d08-16: Trip Great Russia
- 2017m09d01 Titleist 718 My Experience
- 2017m12d23-31: Vienna The Series Trip
- 2018m01d01: JyHorseman Watches Box
- 2018m02d22: My MEVO FlightScope
- 2018m04d13-17: South Vietnam by Weekend Tours
- JyHorseman List (since 2021m10d20)
- 2022m03d12: Benz W211 E240
- 2023m03d03-09: Hokkaido Ice Breaker, Letago
- 2023m07d07: HP Victus 16-d1213TX
- 2010m01d01: HP Pavillion dv6-1111TX
|
| |
|
| | 1 | 2 | 3 | 4 | 5 |
| 6 | 7 | 8 | 9 | 10 | 11 | 12 |
| 13 | 14 | 15 | 16 | 17 | 18 | 19 |
| 20 | 21 | 22 | 23 | 24 | 25 | 26 |
| 27 | 28 | 29 | 30 | 31 | |
|
| |
|
|
|
|
|
|
|
|
2014m06d25: Medicus Golf Training Aids
www.JyHorseman.Bloggang.com
2014m06d25: Medicus Golf Training Aids
�����͡����Թ��蹷���Ҥ�ø�����Ƕ������ ����ػ�ó�֡�������쿪������Ԥ�� (Medicus) �ͺ����ҡ���˹������Ш���ҹ���� �����ҹ��ʹ㨴� �֧���Ѻ�������֡���������ѡ��¡��
����Ѻ�Ը���ҹ �����֡���������������䫷��ʴ������ʹ� ��µ�ͧ�����������ҧ�ԧ㹡�ý֡���ҹ ����



[Table of Contents]


[The Proper Grip]

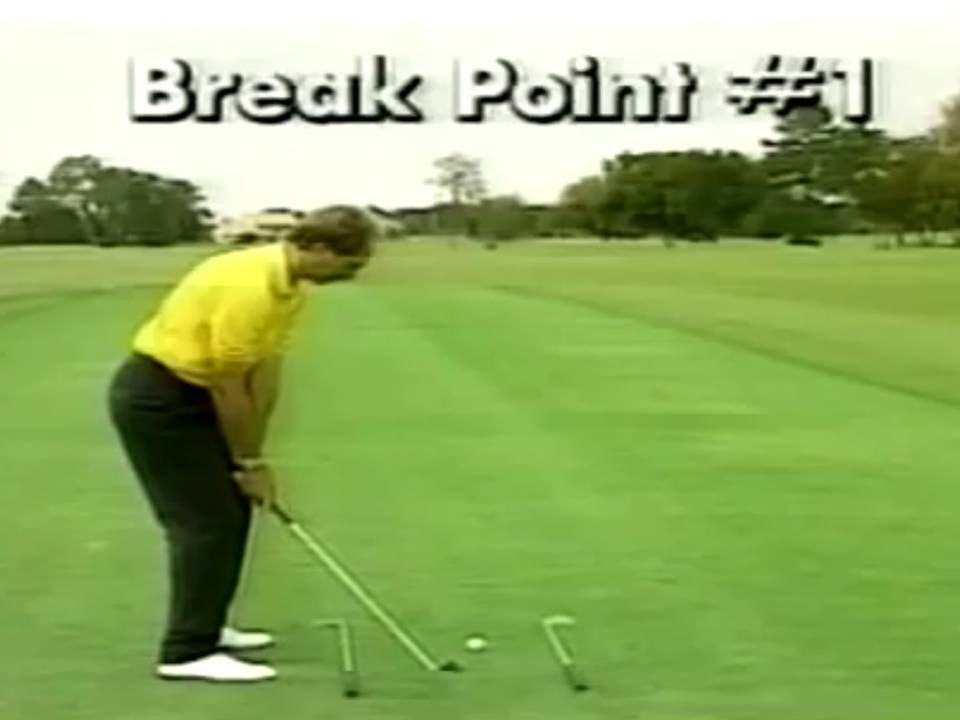
For the correct width of stance the insides of the heels should match the insides of the shoulders. Knees over feet, the right foot turned out 5 degrees and the left foot turned left 10 to 15 degrees.
Weight distributed equally, knees flexed approximately 20 degrees, bending from the stomach area, keeping the hips level and allowing the arms to hang straight down in a relaxed position.
The ball should be placed 2 inches inside the left heel or underneath the left armpit.
Feet, knees, hips, forearms and shoulders are aligned parallel to the target line.

[Posture, Stance & Alignment]
Common Faults:
A. Too much weight on the right side.
B. Hands positioned too far ahead of the ball.
C. Lack of knee bend, hunched over ball, too much bend from the waist.
D. Too much knee flexion, no bending at the hips.


The takeaway is simply rotating your upper body slowly to the right, allowing hands, arms and shoulders to move away together.
This is best accomplished by relaxing the arms and hands and allowing the bigger muscles of the body to begin the movement.
As the one-piece takeaway continues, the hands begin to hinge vertically.

[Breakpoint 1 - Takeaway]
Common Faults:
A. Taking away the club too fast with hinging/cocking of the wrist.
B. Too fast with arms only.
C. Lack of a one-piece takeaway; opening the clubface with the wrist to the inside.
D. Lack of a one-piece takeaway; swinging with the hands pushing the clubface away from the body
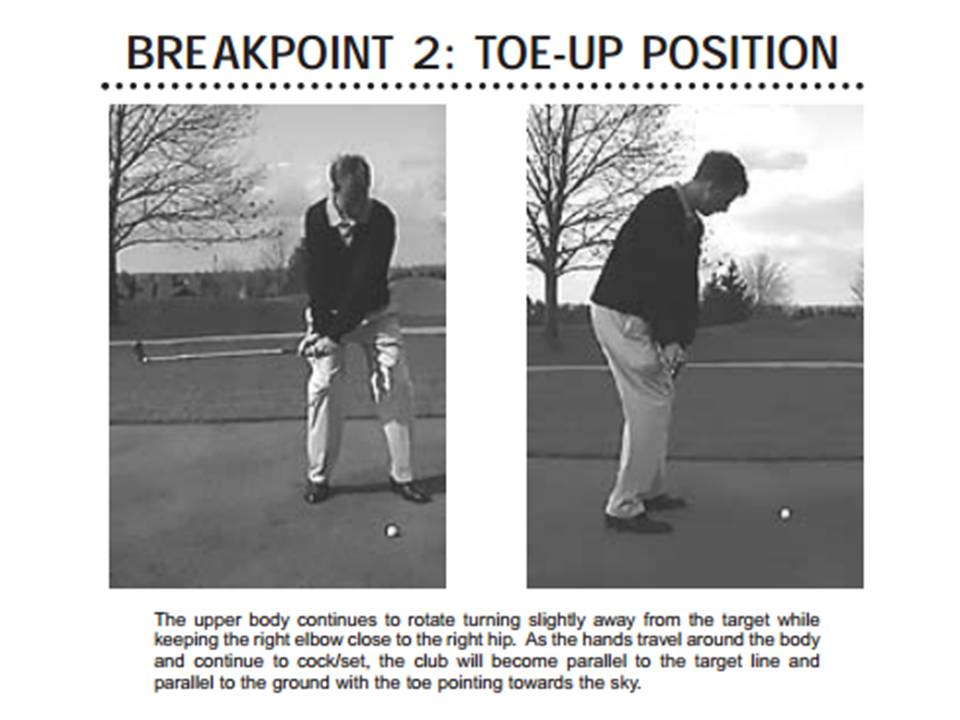
The upper body continues to rotate turning slightly away from the target while keeping the right elbow close to the right hip.
As the hands travel around the body and continue to cock/set, the club will become parallel to the target line and parallel to the ground with the toe pointing towards the sky.
[Breakpoint 2 -Toe-up Position]
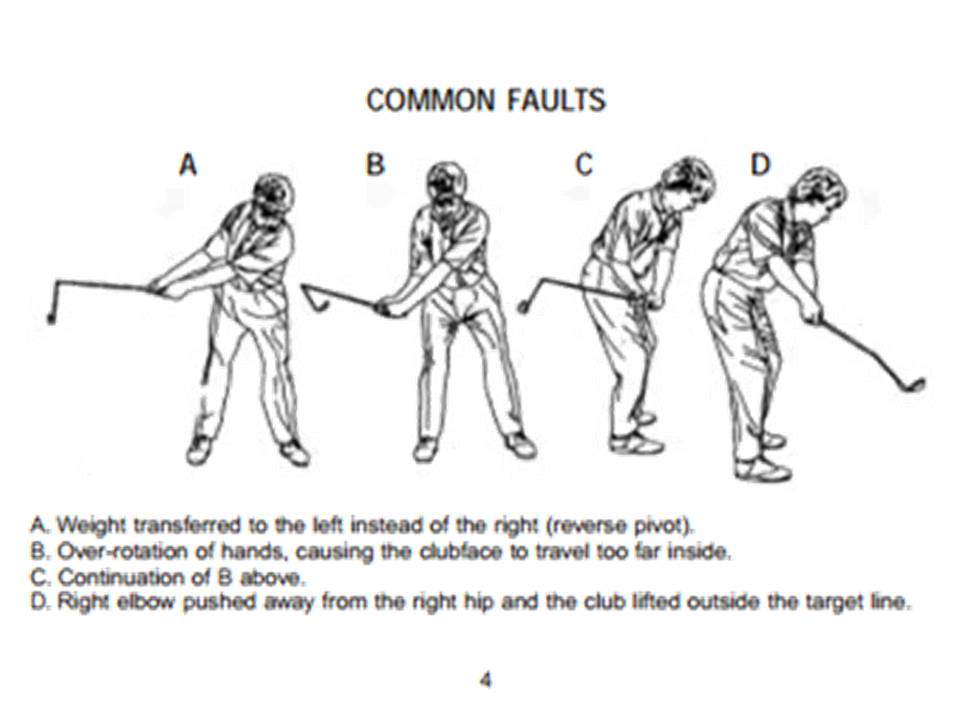
Common Faults:
A. Weight transferred to the left instead of the right (reverse pivot).
B. Over-rotation of hands, causing the clubface to travel too far inside.
C. Continuation of B above.
D. Right elbow pushed away from the right hip and the club lifted outside the target line

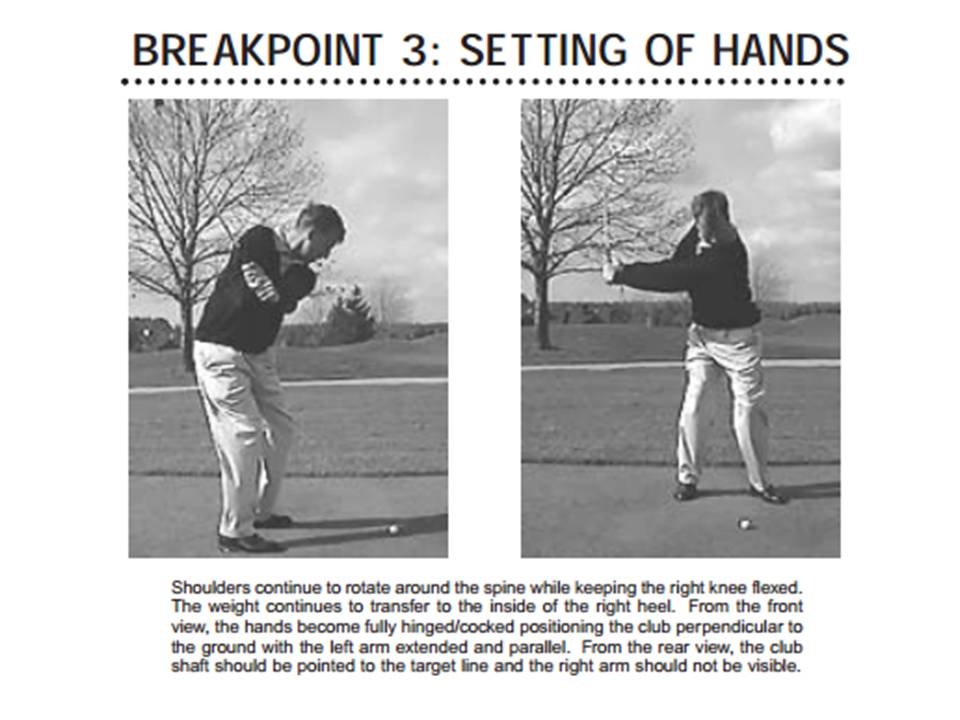
Shoulders continue to rotate around the spine while keeping the right knee flexed.
The weight continues to transfer to the inside of the right heel.
From the front view, the hands become fully hinged/cocked positioning the club perpendicular to the ground with the left arm extended and parallel.
From the rear view, the club shaft should be pointed to the target line and the right arm should not be visible.
[Breakpoint 3 - Setting of Hands]
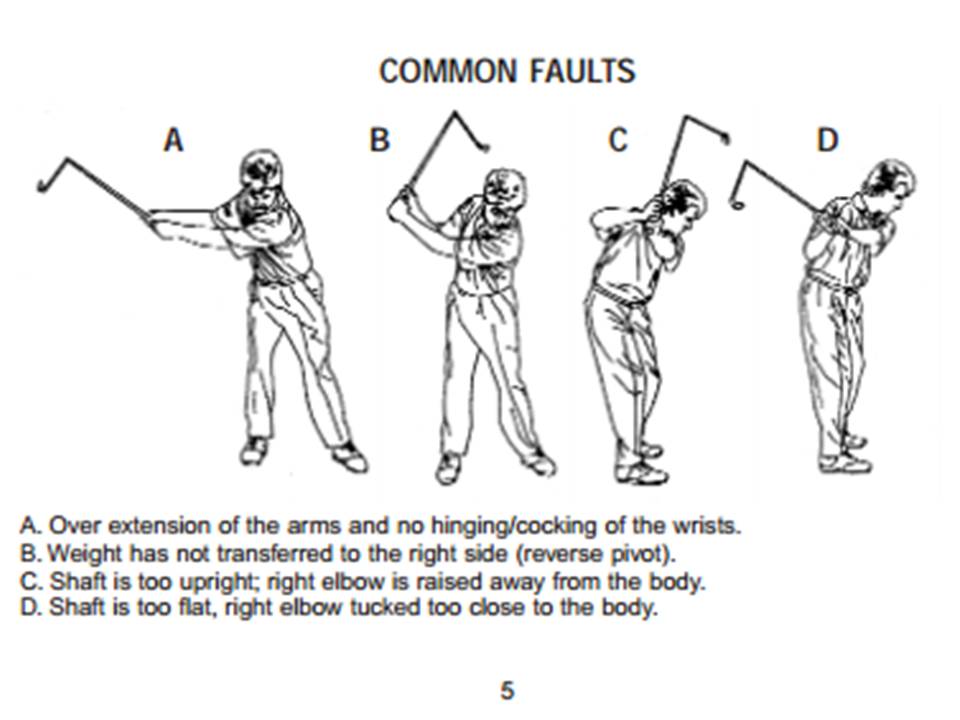
Common Faults:
A. Over extension of the arms and no hinging/cocking of the wrists.
B. Weight has not transferred to the right side (reverse pivot).
C. Shaft is too upright; right elbow is raised away from the body.
D. Shaft is too flat, right elbow tucked too close to the body

At the top of the back swing, your shoulders should be rotated 90 degrees to the target line with your hips at 45 degrees.
The right knee maintains flexed and the left knee points towards the golf ball.
From the rear view, the club should be parallel to the target line with both hands under the shaft for support.
The clubface is in a semi-skyward position and the right forearm should be perpendicular to the ground.

[Breakpoint 4 - At the Top]
Common Faults:
A. Weight has swayed to the outside of the right foot.
B. Weight has remained on the left side.
C. Shaft points right of the target line and the left wrist is cupped, which opens the clubface.
D. Shaft points left of target line and the left wrist is bowed, which closes the clubface.

This is the key to getting distance when hitting the ball.
The Medicus Dual 2000 is unique in that it has a more sensitive angle design so that the least flaw will be detected at this point in the swing.
This does not minimize the importance in maintaining proper positioning as seen through the mechanics enforced by the Medicus, but the Medicus Dual 2000 has the enhancements to enforce your ability to get the greatest distance out of your swing.
As the downswing unwinds, the arms and hands should be accelerating at a faster pace than the body.
This must take place in order for them to get into a position where they can move together with the body through impact.
The right knee momentarily holds its position as the arms accelerate.
As the left arm comes back to parallel position with the ground, the�right elbow should be very close to the body.
Once again, the club shaft is pointing at the target line and the wrists remain fully cocked.

[Breakpoint 5 - Initial Move Down]
Common Faults:
A. Casting the club outward from the top, early unhinging/uncocking of the wrists.
B. Club shaft is dropped to a very flat position caused by trying to swing from too much inside out.

With the hands in from of the body, the club shaft becomes parallel to the target line with the toe of the club skyward.
The wrists continue to remain cocked forming a 90-degree angle with the club shaft and the left forearm.
[Breakpoint 6 - Pre-Impact]
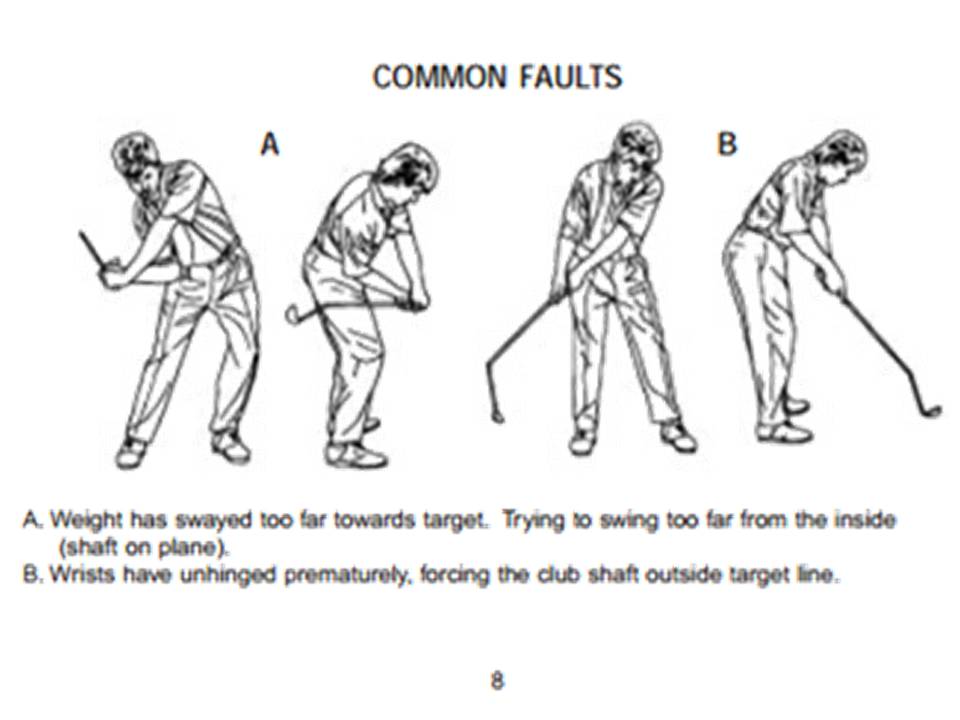
Common Faults :
A. Weight has swayed too far towards target. Trying to swing too far from the inside (shaft on plane).
B. Wrists have unhinged prematurely, forcing the club shaft outside target line.

As the hands, shoulders, hips and body together move into impact, the club is released with the hands ahead of the ball and the clubface square.
Hips will be approximately 30-45 degrees open to the target line and the shoulders about 5 degrees open.
The left leg should be slightly flexed but in the process of�straightening.
Because of the weight shift, the right heel will be pulled slightly off�the ground.
The head remains behind the ball, right arm is extending while the�writs are uncocking.

[Breakpoint 7 - Impact]
Common Faults :
A. Upper body has fallen away from target, no weight shift to the left and no body turn (reverse pivot).
B. Head is in front of the ball. Upper body slides through toward target.

Weight has shifted over to the left side with the hips rotated 80-90 degrees open to the target line.
Club shaft is parallel to the target line and parallel to the ground�with the toe skyward again.
Head remains down and behind the ball with both arms fully extended.
Left leg should be straight at this point to allow the hips to continue turning.

[Breakpoint 8 - Post-Impact]
Common Faults :
A. Both arms are fully extended (right arm is too far away from the body). Head has moved from the impact position.
B. Over rotation of the hands, club shaft is pointing left of the target line. Left arm is fully extended.
C. Continuation of B above.
D. No rotation of the hands, club shaft is facing well right of the target.
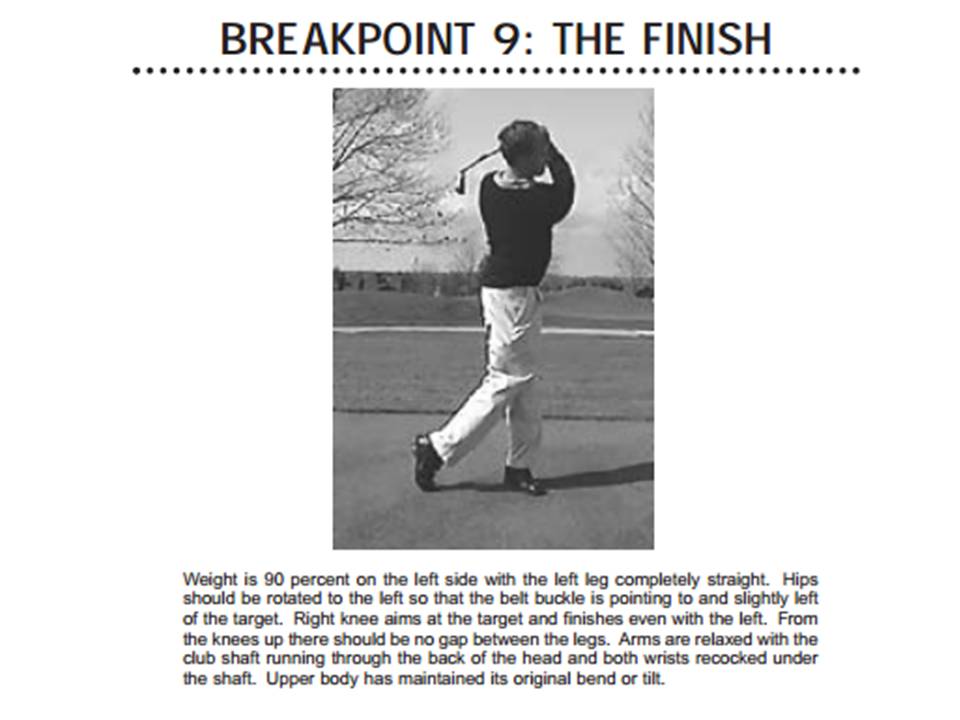
Weight is 90 percent on the left side with the left leg completely straight.
Hips should be rotated to the left so that the belt buckle is pointing to and slightly left of the target.
Right knee aims at the target and finishes even with the left.
From the knees up there should be no gap between the legs.
Arms are relaxed with the club shaft running through the back of the head and both wrists recocked under the shaft.
Upper body has maintained its original bend or tilt.

[Breakpoint 9 - The Finish]
Common Faults :
A. Weight is on the right side, no transfer, rotation stops.
B. Right shoulder dipped well beneath left; back is not in an upright position. Right knee is not even with the left knee.

: Adjustable Tension Hinge :
To set the standard hinge tension, you must check the club's response.
Hold the club parallel to the ground directly in front of you, using one hand.
Align the hinge mechanism so it can break downward allowing the head to fall freely.
The hinge at either position should not break or bend in this position, but remain rigid.
The hinge at both positions should react (by breaking) with a short and quick upward movement of your wrist.
If the hinge fails to break, the tension is set too tight and should be adjusted at either hinge adjustment point.
To make the hinge more responsive or more fluid, turn the setscrew with the included wrench counter-clockwise.
To make the hinge less responsive or less fluid, turn the setscrew clockwise to increase the tension.


��������ҧ�ԧ
- �����͡����ҹ ������-�����ѡ (Medicus/Idea) :
//www.medicus.com/MedicusDual2000Booklet.pdf
- Youtube, Medicus Golf Instruction-Dual Hinge Irons :
https://www.youtube.com/watch?v=zZSg5Z0RlG8

[Youtube, Medicus Golf Instruction-Dual Hinge Irons :
https://www.youtube.com/watch?v=zZSg5Z0RlG8]
- Youtube, The Medicus Dual Hinge Driver - Producing Results :
https://www.youtube.com/watch?v=gu2Kd2wl6wg

[Youtube, The Medicus Dual Hinge Driver - Producing Results :
https://www.youtube.com/watch?v=gu2Kd2wl6wg]
�Ҵ��ѧ��� ��ý֡�Ѵ���쿹�ҨоѲ�Ң���� �ͧ���ͧ���ѡ����
//www.JyHorseman.Bloggang.com
| Create Date : 01 �á�Ҥ� 2557 |
| Last Update : 21 �á�Ҥ� 2557 13:46:24 �. |
|
0 comments
|
| Counter : 2339 Pageviews. |
 |
|
|
|
|
|
|
:Users Online
Jy Horseman
|
| |
|
|
|
|
|
|
|






























 �ҡ��ͤ�����ѧ����
�ҡ��ͤ�����ѧ���� ���Դ������͡ : 5 �� [
���Դ������͡ : 5 �� [