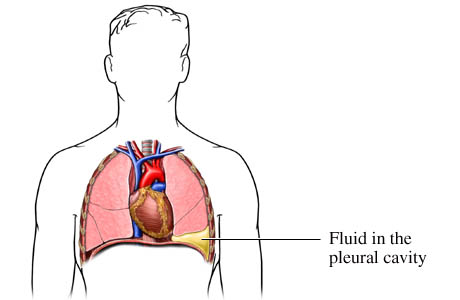
Thoracentesis is a procedure to remove fluid from the space between the lungs and the chest wall called the pleural space. It is done with a needle (and sometimes a plastic catheter) inserted through the chest wall. This pleural fluid may be sent to a lab to determine what may be causing the fluid to accumulate in the pleural space.
Normally only a small amount of pleural fluid is present in the pleural space. Accumulation of excess pleural fluid (pleural effusion) may be caused by many conditions, such as infection, inflammation, heart failure, or cancer. If a large amount of fluid is present, it may be difficult to breathe. Fluid inside the pleural space may be found during a physical examination and is usually confirmed by a chest X-ray.
Why It Is Done Thoracentesis may be done to:
Determine the cause of excess pleural fluid (pleural effusion). Relieve shortness of breath and pain caused by a pleural effusion. How To Prepare You will be asked to sign a consent form before a thoracentesis. Talk to your doctor about any concerns you have regarding the need for the procedure, its risks, how it will be done, or what the results will indicate. To help you understand the importance of this procedure, fill out the medical test information form(What is a PDF document?).
Tell your doctor if you:
Are taking any medications. Have allergies to any medications, including anesthetics. Have any bleeding problems or take blood thinners, such as aspirin or warfarin (Coumadin). Are or might be pregnant. Also, certain conditions may increase the difficulty of thoracentesis. Let your doctor know if you have:
Had lung surgery. The scarring from the first procedure may make it difficult to do this procedure. A long-term (chronic), irreversible lung disease, such as emphysema. A chest X-ray is usually done before the procedure. Your doctor may order certain blood tests, such as a complete blood count (CBC) and bleeding factors, before your procedure.
How It Is Done This procedure may be done in your doctor's office, in the X-ray department of a hospital, in an emergency room, or at your bedside in the hospital. Your doctor may have a nurse assist with the procedure.
You will need to take off all or most of your clothes (you may be allowed to keep on your underwear if it does not interfere with the procedure). You will be given a cloth or paper covering to use during the procedure. During the procedure, you will be seated but leaning forward on a padded bedside table. If your test is done in the X-ray department, X-rays or an ultrasound may be used to confirm the location of fluid in your chest.
How It Is Done continued... The needle site between your ribs will be cleaned with an antiseptic solution. Your doctor will give you a local anesthetic in your chest wall so you won't feel any pain when the longer needle that withdraws the fluid is inserted. Once the area is numb, your doctor will insert the needle to where the fluid has collected (pleural space). You may feel some mild pain or pressure as the needle enters the pleural space.
A syringe or a small tube attached to a vacuum bottle is used to remove the pleural fluid. Your doctor collects 50 mL to 100 mL of fluid at a time to send to the lab. Up to 1500 mL may be removed if the fluid is making it difficult for you to breathe. Once the fluid is removed, the needle or small tube is removed and a bandage is put on the site.
An X-ray is usually taken right after the procedure to make sure that no complications have occurred. If more pleural fluid collects and needs to be removed, another thoracentesis may be done later.
This procedure takes about 10 to 15 minutes.
How It Feels When you are given the shot to numb your skin at the needle site, you will feel a sharp stinging or burning sensation that lasts a few seconds. When the needle is inserted into the chest wall, you may again feel a sharp pain for a few seconds.
When the pleural fluid is removed, you may feel a sense of "pulling" or pressure in your chest. Tell your doctor or nurse if you feel faint or if you have any shortness of breath, chest pain, or uncontrollable cough.
If a large amount of pleural fluid was removed during the procedure, you will probably be able to breathe more easily.
Risks Thoracentesis is generally a safe procedure. A chest X-ray is usually done right after the procedure to make sure that no complications have occurred. Complications may include:
A partial collapse of the lung (pneumothorax). This may occur if the needle used to remove the pleural fluid punctures the lung, allowing air to flow into the pleural space. Pulmonary edema, which may occur if a large amount of fluid is removed. Infection and bleeding. Damage to the liver or spleen, though this is rare.
Results Thoracentesis is a procedure to remove fluid from the space between the lungs and the chest wall called the pleural space. Results from a lab are usually available in 1 to 2 working days. If the fluid is being tested for an infection, such as tuberculosis, results may not be available for several weeks.
What Affects the Test Factors that can interfere with your procedure or the accuracy of the results include:
Use of antibiotics. The inability to remain still. What To Think About Thoracentesis may not be done for people who have: A bleeding disorder. Heart failure or enlargement of the right side of the heart (cor pulmonale). A pleural biopsy may be done at the same time as a thoracentesis to collect a sample of tissue from the inner lining of the chest wall. Thoracentesis may be done before another procedure called pleurodesis. During this procedure, a chemical or medication (talc or doxycycline) is put into the pleural space, which triggers an inflammatory reaction over the surface of the lung and inside the pleural space. This in turn causes the layer of pleura attached to the lung to stick to the layer of pleura on the inside of the chest wall. This takes away the space between the pleura and prevents or reduces the collection of more pleural fluid. Pleurodesis may be done when fluid collects in the chest more than one time.
Other Works Consulted Chernecky CC, Berger BJ, eds. (2004). Laboratory Tests and Diagnostic Procedures, 4th ed. Philadelphia: Saunders.
Fischbach FT, Dunning MB III, eds. (2004). Manual of Laboratory and Diagnostic Tests, 7th ed. Philadelphia: Lippincott Williams and Wilkins.
Pagana KD, Pagana TJ (2006). Mosbys Manual of Diagnostic and Laboratory Tests, 3rd ed. St. Louis: Mosby.
Thoracentesis (also known as thoracocentesis or pleural tap) is an invasive procedure to remove fluid or air from the pleural space for diagnostic or therapeutic purposes. A cannula, or hollow needle, is carefully introduced into the thorax, generally after administration of local anesthesia. The procedure was first described in 1852.
The recommended location varies depending upon the source. Some sources recommend the midaxillary line, in the sixth, seventh, or eighth intercostal space.[1]
Indications This procedure is indicated when unexplained fluid accumulates in the chest cavity outside the lung. In more than 90% of cases analysis of pleural fluid yields clinically useful information. If a large amount of fluid is present, then this procedure can also be used therapeutically to remove that fluid and improve patient comfort and lung function.
The most common causes of pleural effusions are cancer, congestive heart failure, pneumonia, and recent surgery. In countries where tuberculosis is common, this is also a common cause of pleural effusions.
When cardiopulmonary status is compromised (i.e. when the fluid or air has its repercussions on the function of heart and lungs), due to air (significant pneumothorax), fluid (pleural fluid) or blood (hemothorax) outside the lung, then this procedure is usually replaced with tube thoracostomy, the placement of a large tube in the pleural space.
Contraindications An uncooperative patient or a coagulation disorder that can not be corrected are absolute contraindications.
Relative contraindications are site of insertion has known bullous disease (e.g. emphysema), use of positive end-expiratory pressure (PEEP, see mechanical ventilation) and only one functioning lung (due to diminished reserve).
Complications Major complications are pneumothorax (3-30%), hemopneumothorax, hemorrhage, hypotension (low blood pressure due to a vasovagal response) and reexpansion pulmonary edema.
Minor complications include a dry tap (no fluid return), subcutaneous hematoma or seroma, anxiety, dyspnea and cough (after removing large volume of fluid).
Interpretation of pleural fluid analysis Several diagnostic tools are available to determine the etiology of pleural fluid.
Transudate versus exudate First the fluid is either transudate or exudate.
A transudate is defined as pleural fluid to serum total protein ratio of less than 0.5, pleural fluid to serum LDH ratio < 0.6, and absolute pleural fluid LDH < 200 IU or < 2/3 of the normal serum level.
An exudate is any pleural fluid that does not meet aforementioned criteria.
Amylase A high amylase level (twice the serum level or the absolute value is greater than 160 Somogy units) in the pleural fluid is indicative of either acute or chronic pancreatitis, pancreatic pseudocyst that has dissected or ruptured into the pleural space, cancer or esophageal rupture.
Glucose This is considered low if pleural fluid value is less than 50% of normal serum value. The differential diagnosis for this is: - rheumatoid effusion - lupus effusion - bacterial empyema - malignancy - tuberculosis - esophageal rupture (Boerhaave syndrome)
pH Normal pleural fluid pH is approximately 7.60. A pleural fluid pH below 7.30 with normal arterial blood pH has the same differential diagnosis as low pleural fluid glucose.
Triglyceride and cholesterol Chylothorax (fluid from lymph vessels leaking into the pleural cavity) may be identified by determining triglyceride and cholesterol levels, which are relatively high in lymph. A triglyceride level over 110 mg/dl and the presence of chylomicrons indicate a chylous effusion. The appearance is generally milky but can be serous.
The main cause for chylothorax is rupture of the thoracic duct, most frequently as a result of trauma or malignancy (such as lymphoma).
Cell count and differential The number of white blood cells can give an indication of infection. The specific subtypes can also give clues as to the type on infection. The amount of red blood cells are an obvious sign of bleeding.
Cultures and stains If the effusion is caused by infection, microbiological culture may yield the infectious organism responsible for the infection, sometimes before other cultures (e.g. blood cultures and sputum cultures) become positive. A Gram stain may give a rough indication of the causative organism. A Ziehl-Neelsen stain may identify tuberculosis or other mycobacterial diseases.
Cytology Cytology is an important tool in identifying effusions due to malignancy. The most common causes for pleural fluid are lung cancer, metastasis from elsewhere and mesothelioma. The latter often presents with an effusion. Normal cytology results do not reliably rule out malignancy, but make the diagnosis more unlikely.
References ^ Human Gross Anatomy. Retrieved on 2007-10-22. - Intensive Care Medicine by Irwin and Rippe - The ICU Book by Marino - Procedures and Techniques in Intensive Care Medicine by Irwin and Rippe - Pulmonary - Critical Care Associates of East Texas - Thoracentesis from THE MERCK MANUAL, Sec. 6, Ch. 65, Special Procedures
External links - A photo gallery of thoracentesis showing the procedure step-by-step. V. Dimov, B. Altaqi, Clinical Notes, 2005. A free PDA version. - Diagnostic Thoracentesis Virtual Cancer Centre - Therapeutic Thoracentesis Virtual Cancer Centre





 ฝากข้อความหลังไมค์
ฝากข้อความหลังไมค์ ผู้ติดตามบล็อก : 84 คน [
ผู้ติดตามบล็อก : 84 คน [